Timing of inspiratory muscle activity detected from airway pressure and flow during pressure support ventilation: the waveform method
We are the Editor’s Pick!
See how to use ventilator waveforms to reliably assess patient’s spontaneous activity and patient–ventilator interaction! Full text here on Critical Care
Abstract
Background
Whether respiratory efforts and their timing can be reliably detected during pressure support ventilation using standard ventilator waveforms is unclear. This would give the opportunity to assess and improve patient–ventilator interaction without the need of special equipment.
Methods
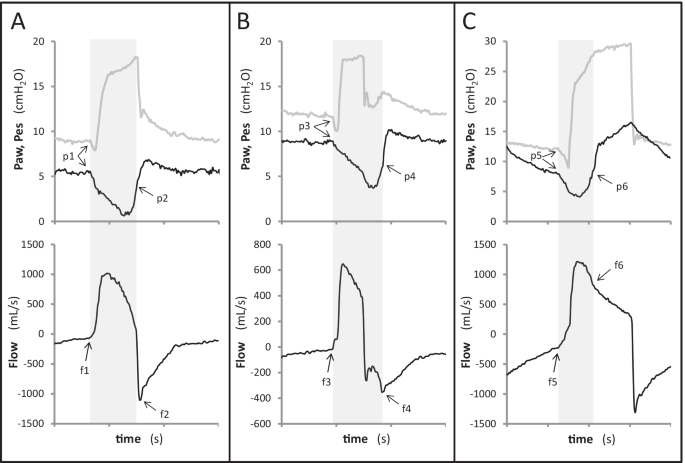
In 16 patients under invasive pressure support ventilation, flow and pressure waveforms were obtained from proximal sensors and analyzed by three trained physicians and one resident to assess patient’s spontaneous activity. A systematic method (the waveform method) based on explicit rules was adopted. Esophageal pressure tracings were analyzed independently and used as reference. Breaths were classified as assisted or auto-triggered, double-triggered or ineffective. For assisted breaths, trigger delay, early and late cycling (minor asynchronies) were diagnosed. The percentage of breaths with major asynchronies (asynchrony index) and total asynchrony time were computed.
Results
Out of 4426 analyzed breaths, 94.1% (70.4–99.4) were assisted, 0.0% (0.0–0.2) auto-triggered and 5.8% (0.4–29.6) ineffective. Asynchrony index was 5.9% (0.6–29.6). Total asynchrony time represented 22.4% (16.3–30.1) of recording time and was mainly due to minor asynchronies. Applying the waveform method resulted in an inter-operator agreement of 0.99 (0.98–0.99); 99.5% of efforts were detected on waveforms and agreement with the reference in detecting major asynchronies was 0.99 (0.98–0.99). Timing of respiratory efforts was accurately detected on waveforms: AUC for trigger delay, cycling delay and early cycling was 0.865 (0.853–0.876), 0.903 (0.892–0.914) and 0.983 (0.970–0.991), respectively.
Conclusions
Ventilator waveforms can be used alone to reliably assess patient’s spontaneous activity and patient–ventilator interaction provided that a systematic method is adopted.